The Inflation Reduction Act: The Devil is in the Details for Patients with Rare Diseases
David Gibson, PhD, CMPP
Director of Strategic Programs, Engagement, and Communications
Amyloidosis Research Consortium

The Inflation Reduction Act (IRA), signed into law on August 16, 2022, tackled a wide range of issues from tax reform, energy security, environmental and agricultural protection, all the way to climate change. The world of health care was not left untouched, and the IRA included specific efforts to reduce the prices of prescription drugs – an effort with obvious wide-spread support across families in the United States.
The IRA requires The Centers of Medicare and Medicaid Services (CMS) to negotiate the prices of certain high-cost prescription drugs covered under Medicare starting in 2026. Initially, only 10 drugs that are paid for under Medicare Part D (drugs you get at the pharmacy, or another retail location) are eligible for negotiation, but this number will increase each subsequent year. In addition, beginning in 2028, drugs covered under Medicare Part B (drugs you get in a doctor’s office, hospital, or an out-patient infusion center) will also become eligible for price negotiation. So far so good. But while trying to lower drug prices is a laudable aim, it may come at the unintended cost of future innovation of new orphan drugs (therapies for “rare diseases,” that is diseases that impact fewer than 200,000 individuals).
The Impact of Rare Diseases
First, let’s quickly talk about rare diseases. More than 7,000 rare diseases impact more than 30 million people in the United States. Many of these are children. And this challenging situation is further compounded by the fact that approximately 95% of rare diseases do not have an FDA-approved treatment. As a result, FDA has announced that a key priority is to support the development of orphan drugs and to this end, FDA has the authority to grant orphan drug designation to a drug or biological product early in the development process. This designation qualifies the drug development company to unlock several incentives, including tax credits and grants for new research. Developing a drug for a rare disease is hard – the disease is often not well understood, patient numbers are typically small, and the roadmap of how to design a successful clinical trial can be unclear at best. Consequently, the incentives granted with orphan drug designation are essential for companies in this space. And it has worked, with over 650 orphan drugs approved since the passage of the Orphan Drug Act in 1983.
“More than 7,000 rare diseases impact more than 30 million people in the United States…and approximately 95% of rare diseases do not have an FDA-approved treatment.”
Potential Negative Consequences of the IRA
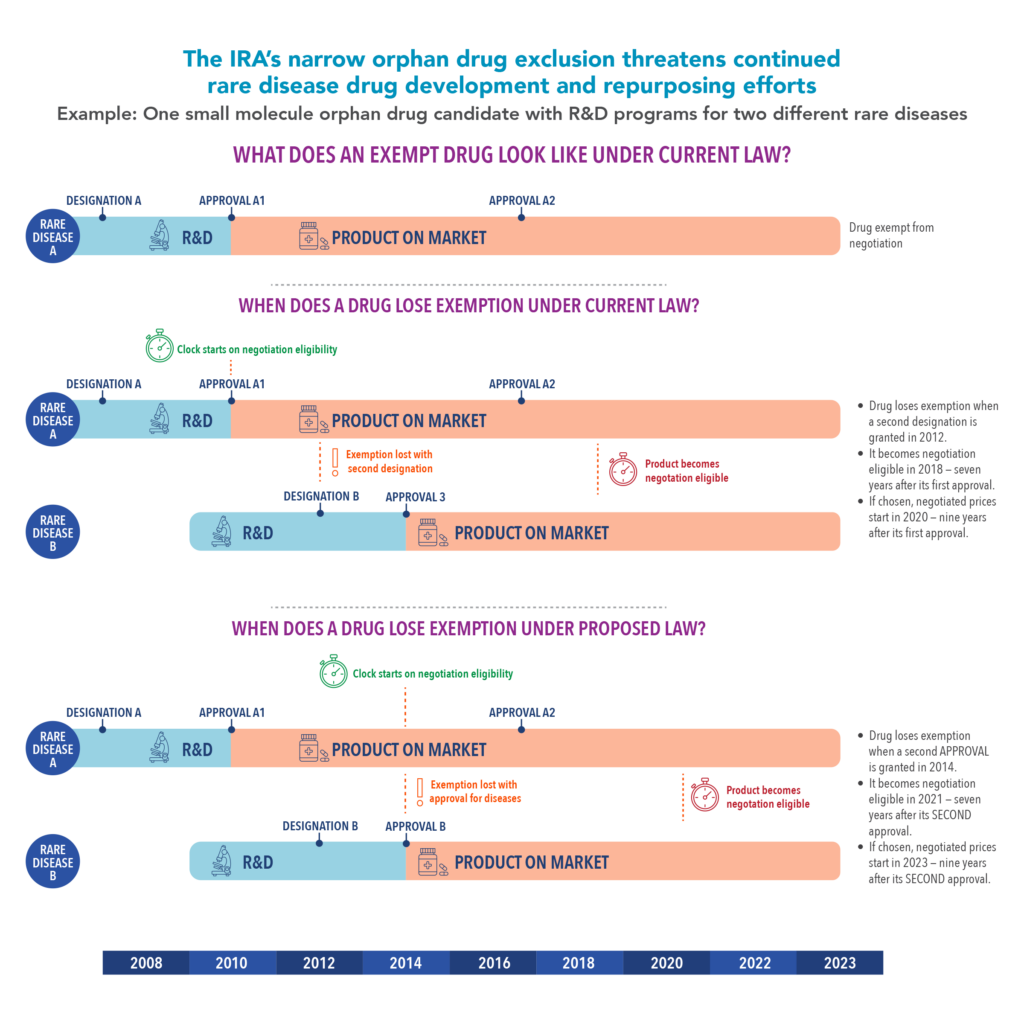
Now-back to the IRA. The IRA exempts orphan drugs, like those approved for amyloidosis, from price negotiations, although this exemption applies only to orphan drugs with a single approved indication (approved to treat a single disease or illness), a move intended to incentivize companies to develop drugs for rare diseases. However, as the saying goes, “the devil is in the details” and as stated above, the exemption applies only to orphan drugs with a single approved indication. As soon as such a drug is granted a second designation for another rare disease the exemption is lost and the drug could be subject to price controls. What does this mean for rare diseases? Companies might not seek approval for a new drug to treat multiple diseases.
It is important to remember that drug developers often continue research on approved products for other indications, and there are many situations where a drug approved for one disease can work well in another disease. Indeed, between 2003 and 2022, FDA approved approximately a quarter of orphan drugs for at least one additional disease, or “follow-on indication” (Chambers JD, Clifford KA, and Enright DE. JAMA Netw Open, 2023). What would this number be if the incentive to study an approved drug in an additional disease was removed? What will companies do if they are unlikely to see a return on their investment? Combined with other challenges in rare drug development, are we creating a hostile environment for orphan drug development? The individuals that pay the ultimate price are the patients and families.
“Drug developers often continue research on approved products for other indications, and there are many situations where a drug approved for one disease can work well in another disease. Indeed, between 2003 and 2022, FDA approved approximately a quarter of orphan drugs for at least one additional disease.”
So, let’s talk about a real-life consequence involving a drug well known to the amyloidosis community – Amvuttra™, currently approved to treat the polyneuropathy caused by hereditary ATTR amyloidosis. Alnylam Pharmaceuticals has been evaluating Amvuttra for Stargardt Disease, a rare eye disease that can result in vision loss. However, they announced in 2022 they would not start a Phase 3 trial of Amvuttra in Stargardt patients as previously announced, blaming the IRA and the potential for price negotiation with a second orphan drug designation.
Small Changes For A Big Improvement
How do we fix this situation? While we do need to acknowledge that there may be little appetite in Congress for big changes to the IRA, there are some fixes that can be made that will certainly help.
First, Congress must clarify that the number of orphan drug designations that FDA grants to a product has no effect on its eligibility to be exempt from price negotiations. We need to expand the orphan drug exemption beyond drugs approved for only one rare disease.
Second, we need to clarify that an orphan drug becomes price negotiation eligible 7 years (for small molecule drugs) or 11 years (for biologics) after it loses that exemption. This will allow science and patient need to drive drug development companies’ investment in a rare disease rather than the price negotiation timeline.
Driven by amazing advances in the understanding of many rare diseases, the science and technology behind the development of novel therapies, and herculean efforts by patient advocacy groups, new hope has been brought to many rare disease communities. While the cost of prescription drugs is a major issue for patients and their families and must be addressed, we should be careful not to simultaneously impact the ability of companies to develop therapies in the rare disease space.
- Categories